
A couple of weeks ago, the final results from the DESTINY trial were presented at EHA (European Hematology Association).
You can find the abstract of the presentation here.
The key points were:
- TKI treatment was de-escalated to 50% of the standard dose (imatinib 200mg daily, dasatinib 50mg daily or nilotinib 200mg twice daily) for 12 months, then stopped altogether for a further 24 months.
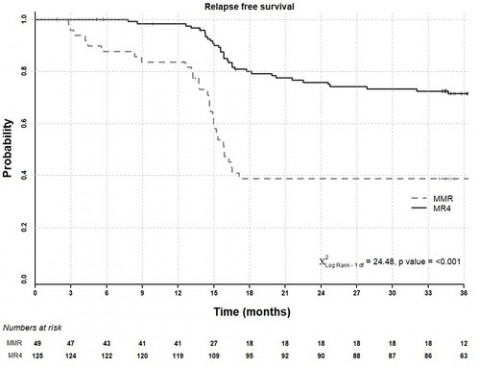
- 72% of patients who were at MR4 at entry have been able to remain in treatment free remission
- 39% of patients who were at MMR (MR3) at entry have been able to remain in treatment free remission
- There was no difference in those at MR4 and those at MR4.5 at entry
- It seems that initial de-escalation is not simply delaying recurrence, though the mechanism of its benefit is not yet clear. Possibilities include gradual mobilisation of leukaemic stem cells into cycle and/or gradual improvement in the anti-leukaemic immune response at a time when TKI is still present. These require further study.
For those who like a graph:
David

